

Last updated: June 2026. BPC-157 and TB-500 are research-stage peptides, not FDA-approved finished drugs, and the human evidence for using them together is close to nonexistent. Every claim here links to a primary source, so you don’t have to take my word for anything.
Here’s a question worth asking about any two-ingredient combination somebody hands you at the gym: has anyone actually tested the combination, or have they just tested the two ingredients separately and assumed they’d play nice together? That question is the whole spine of this article, because when I went looking for proof that the so-called “repair stack” (BPC-157 plus TB-500) actually works, I found something closer to a guess wearing a lab coat.
Let me walk you through it the way I’d explain it to a friend who’s never heard either name before.
First, what are these two things, actually?
Think of a peptide as a short strand of amino acids, the building blocks that also link up into full proteins, just shorter. Peptides are made in a lab to mimic something the body already makes, or a piece of something the body already makes. That distinction between “the whole thing” and “a piece of it” turns out to matter a lot here, so hang onto it.
BPC-157 is a synthetic peptide. The name stands for “body protection compound,” and it’s modeled on a fragment found in human gastric juice, the fluid your stomach uses to digest food. The original research asked whether this fragment could help protect and heal tissue in the gut. Interest later spread outward to tendons, ligaments, and muscle, which is how it wound up in gym locker conversations instead of gastroenterology textbooks.
TB-500 is a synthetic fragment of a naturally occurring peptide called thymosin beta-4. Notice the word “fragment” again. TB-500 is not thymosin beta-4. It’s a smaller piece being sold as a stand-in for the real thing. That’s a bit like selling someone a single gear from a watch and calling it a watch. It might do something. It is not the same object the good research was done on.
Neither peptide is a vitamin, a supplement, or an approved medication. Both are typically sold online as “research chemicals,” a legal label meaning “for research use only, not for human consumption.” That label describes what the seller is permitted to claim, not what buyers actually do with the vial once it arrives. That gap, between the label and the actual use, turned out to be the most important fact in this whole story.
The pitch: why stack two things instead of one?
I want to give the theory a fair hearing before I poke holes in it, because it isn’t a dumb idea on its face.
The argument goes: BPC-157 and TB-500 are both thought to support tissue repair, but supposedly through different biological routes. Combine them, the thinking goes, and you cover more ground than either one alone, healing faster and more completely. Fans call it the repair stack, or, in its more excitable branding, the “Wolverine stack.” It’s the most-searched peptide pairing there is.
That’s not a crazy instinct. Real medicine does this all the time. Doctors combine two drugs that hit a disease from different angles because the combination has been tested and shown to outperform either one alone. The flaw here isn’t the logic. It’s that nobody ran the actual experiment. Real combination therapy tests the combination. This pairing was assembled from diagrams of how each peptide is thought to work, then sold to you as if the word “additive” were a finding instead of a hope.
What the evidence actually shows, once you go look
This is where my search stopped feeling like research and started feeling like watching a house of cards.
BPC-157’s evidence: mostly cells and rats, barely any people
The reputation BPC-157 has for healing tendons comes almost entirely from preclinical work, meaning lab dishes and animals, not humans. The most frequently cited tendon study, published in the Journal of Applied Physiology in 2011, found that BPC-157 helped cultured tendon cells grow, survive stress, and migrate through a specific cellular pathway [S1]. That’s a genuine, carefully done result. It’s also cells in a dish and rats in a cage, not a person with a sore shoulder.
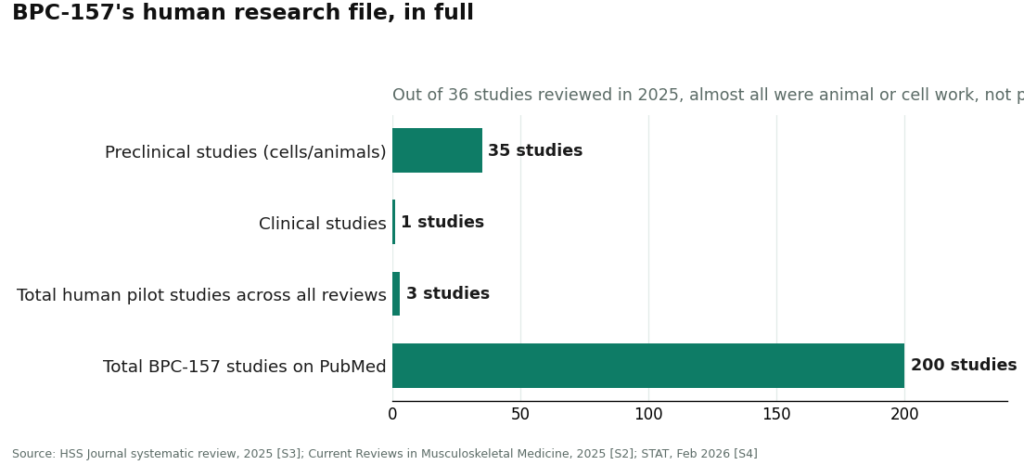
So I looked for the human data, and this is where things got thin fast. A 2025 systematic review in the HSS Journal examined 36 BPC-157 studies. Thirty-five were preclinical. Exactly one was clinical, involving 12 patients, and the reviewers concluded that no clinical safety data existed for the compound [S3]. A separate 2025 review, in Current Reviews in Musculoskeletal Medicine, arrived at nearly the same spot from a different angle: only three small pilot studies have ever looked at BPC-157 in actual humans, covering knee pain, interstitial cystitis, and a basic IV safety check [S2]. Three pilots. That is the entire human research file behind a compound plenty of people talk about like it’s settled science.
One more wrinkle surprised me. Reporting from STAT in February 2026 found that the large majority of the roughly 200 BPC-157 studies indexed on PubMed trace back to a single research group, raising real questions about whether the findings have ever been independently confirmed [S4]. The same article quoted Flynn McGuire, chief medical resident at University of Utah Health, who put it bluntly: “the amount of hype to evidence is just so skewed, it’s crazy.” His personal view was that the compound “should not be used by humans” [S4]. When almost every study traces to one lab, and almost none of it is in people, the word “studied” is doing a lot more marketing work than scientific work.
TB-500’s evidence: real science, wrong molecule
Here’s where the search got sneaky in a way I didn’t expect.
The foundational science behind thymosin beta-4, the parent molecule, is genuinely solid. A 1991 paper in the Journal of Biological Chemistry showed that thymosin beta-4 is essentially the cell’s main actin-sequestering peptide, meaning it locks onto a building-block protein called actin and helps regulate how cells assemble and take apart their internal scaffolding [S5]. Since cell movement and healing both depend on that scaffolding, there’s a real, plausible mechanism there. A 2006 study in the Journal of Cellular Physiology found that thymosin beta-4 boosted certain wound-repair enzymes several-fold in cell and animal models [S6]. So far, that’s a legitimately promising molecule.
But read the label carefully, because the marketing counts on you skimming past it. All of that strong evidence is about thymosin beta-4, the complete natural peptide. TB-500 is the synthetic fragment sold as its substitute. Going from “the parent molecule regulates actin and helps animal wounds” to “this injectable fragment will heal your hamstring” is a leap the sellers make quietly and hope you don’t notice. There is no body of controlled human trials behind injectable TB-500 for soft-tissue repair. The good science belongs to a molecule that isn’t actually what’s in the vial you’re buying.
The stack itself: the one question nobody has answered
So, the actual question: does combining the two beat using either one alone? Here’s the short, honest answer. There is no controlled human trial showing BPC-157 plus TB-500 outperforms BPC-157 alone, TB-500 alone, or plain rest and physical therapy, for any injury, at any dose, in anyone. Zero. The “faster, more complete recovery” language attached to the repair stack comes from seller blogs and forum stories, not from a single study that actually compared the combination to anything.
Stack up the three findings and the picture is stark. BPC-157’s human evidence is nearly empty. TB-500 is a fragment borrowing its reputation from a better-studied relative. And the one claim that’s actually the reason people combine them, the synergy, has never been tested in a human being. It’s two individually under-proven ingredients, sold as if the recipe itself had been taste-tested. It hasn’t.
What to watch for before you consider this
If you’re a competitive athlete in a tested sport, this decision is already made for you before you even get to weigh the evidence. The U.S. Anti-Doping Agency lists BPC-157 as prohibited under the WADA Prohibited List, and TB-500, being a thymosin beta-4 fragment, falls under the growth-factor category the list also restricts [S7]. A “research use only” sticker on the vial protects a tested athlete from exactly nothing.
There’s also the plain matter of not knowing what’s actually in the bottle. Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, told STAT the problem directly: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [S4]. That’s not a scare tactic. It’s a description of an unregulated supply chain with no pharmacy, no testing requirement, and no one accountable if the contents don’t match the label.
How to actually decide
Here’s the reframe I landed on after doing all this reading. The real decision isn’t “which peptide” or “where’s it cheapest.” It’s whether a licensed clinician is anywhere in the process at all.
Buying from a research-chemical site gets you a powder, a legal disclaimer, and nothing else. Nobody reviews your medical history. Nobody checks whether this makes sense next to whatever else you’re taking. No pharmacy stands behind what’s actually in the vial. Nobody is reachable if something goes sideways.
The supervised alternative exists specifically to close that gap. A licensed telehealth provider such as FormBlends handles these peptides the way a real medication is supposed to reach a patient: a physician reviews your history, a prescription gets written when it’s appropriate, and a licensed pharmacy compounds and dispenses the product instead of a warehouse shipping a chemical with a warning label stapled on. That process doesn’t make the repair stack proven. An honest provider will tell you that plainly. What it adds is the layer of accountability that the gray market simply doesn’t have built in.
Where I landed
I didn’t buy the vials. Not because I’m certain the repair stack does nothing at all, but because I went looking for proof that it does something specific, and that proof isn’t there yet. BPC-157’s human evidence amounts to three small pilot studies sitting inside a literature dominated by one research group [S2][S3][S4]. TB-500 is a fragment coasting on a better-studied relative’s credentials [S5][S6]. And the combination, the actual thing being marketed and sold, has exactly zero controlled human trials behind it.
If you read all of that and still want to try it, the honest move is to treat it like the experiment it genuinely is, and to put a licensed clinician between you and the syringe instead of a checkout page and a “research use only” sticker.
Questions people actually ask
Does any human study show the BPC-157 and TB-500 combination works?
No. There’s no controlled human trial showing the combination beats either peptide alone, or beats rest and rehab, for any injury at any dose. The “faster recovery” claim traces back to seller blogs and forum posts, not a single published comparison. Treat the synergy pitch as an idea nobody has tested yet.
What’s the actual difference between TB-500 and thymosin beta-4?
Thymosin beta-4 is the complete natural peptide, and the solid actin-regulating and wound-repair science belongs to that molecule [S5][S6]. TB-500 is a shorter synthetic fragment sold as a stand-in. The marketing leans on the parent molecule’s good reputation, but controlled human evidence for injectable TB-500 in soft-tissue repair simply doesn’t exist.
How much human evidence actually exists for BPC-157?
Very little. A 2025 systematic review of 36 BPC-157 studies found that 35 were preclinical and only 1 was clinical, involving 12 patients, with no clinical safety data reported [S3]. A separate 2025 review counted just three small pilot human studies total [S2]. Most of the roughly 200 papers on PubMed also trace back to one research group, which leaves the question of independent replication wide open [S4].
Could this stack cost me a drug test?
Yes, if you compete in a tested sport. The U.S. Anti-Doping Agency lists BPC-157 as prohibited under the WADA Prohibited List, and TB-500 falls under the growth-factor category the same list restricts [S7]. A “research use only” label offers zero protection to a tested athlete.
Why does it matter that these are sold as “research chemicals”?
Because that label comes with a powder and a disclaimer and nothing else. Nobody reviews your history, no pharmacy is accountable for the contents, and you have no way to confirm what’s actually in the vial. A USADA science officer told STAT the bottle “could be a peptide. It could be a steroid. It could be something just like water” [S4]. Going through a supervised provider like FormBlends adds physician review and pharmacy accountability that the gray market simply doesn’t offer, though it still doesn’t make the stack itself proven.
How do people actually dose BPC-157 and TB-500 together?
There’s no clinically validated dosing protocol for humans, so whatever you read is extrapolated from rodent studies or forum anecdote. The numbers circulating typically run 250 to 500 mcg of BPC-157 once or twice daily, and 2 to 2.5 mg of TB-500 twice weekly during a loading phase, dropping to once weekly after four weeks. None of that is proven safe or effective in people, and copying someone else’s protocol is a real gamble given how much individual physiology varies.
How do you reconstitute a pre-mixed BPC-157 and TB-500 vial?
Most blend vials get reconstituted by slowly injecting bacteriostatic water along the inside wall of the vial, never straight onto the powder, then swirling gently instead of shaking. The amount of water you add determines your concentration per unit drawn, so you need to do that math before drawing up anything. Sterility matters enormously here, and without pharmacy-grade preparation and testing, you can’t actually confirm what’s in the vial or whether it’s degraded.
Is the “Wolverine stack” a different thing?
No, it’s a nickname the fitness world gave the same BPC-157 plus TB-500 combination, riffing on the idea of super-fast healing. Same stack, catchier name. It doesn’t reflect any special formulation, and it carries exactly as much clinical backing as the two peptides do on their own, which is to say, not much.
Can you get these through a legitimate medical route instead of a research-chemical site?
Yes. Compounding pharmacies working under physician supervision, such as FormBlends, can prepare these peptides for patients with a valid prescription, which brings oversight, third-party testing, and accountability a research-chemical seller simply can’t offer. Whether a physician will actually prescribe them depends on your situation and their clinical judgment. It costs more and takes longer, but at least you know what you’re injecting.
References
- Chang CH, Tsai WC, et al. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. Journal of Applied Physiology, 2011. In-vitro and rat study. https://pubmed.ncbi.nlm.nih.gov/21030672/
- Regeneration or risk? A narrative review of BPC-157 for musculoskeletal healing. Current Reviews in Musculoskeletal Medicine, 2025. Human data extremely limited; only three pilot human studies exist (knee pain, interstitial cystitis, IV safety). https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Emerging use of BPC-157 in orthopaedic sports medicine: a systematic review. HSS Journal, 2025. Reviewed 36 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found.
- Safi R, et al. Thymosin beta 4 and Fx, an actin-sequestering peptide, are indistinguishable. Journal of Biological Chemistry, 1991. Thymosin beta-4 forms a 1:1 complex with actin monomers and regulates actin assembly.
- Thymosin beta-4 promotes matrix metalloproteinase expression during wound repair; increased MMP-2 and MMP-9 several-fold over control on day 2; cell and animal models. Journal of Cellular Physiology, 2006.
- Roughly 200 PubMed BPC-157 studies trace largely to a single research group; confirmation-bias and replication concerns; named-expert quotes from Flynn McGuire and Matthew Fedoruk. STAT, Feb 3, 2026.
- U.S. Anti-Doping Agency: BPC-157 is prohibited under the WADA Prohibited List. USADA, 2026.


